
How will weight-loss drugs change our relationship with food?
The rise of these treatments has major implications for how we think about obesity, says James Gallagher.
 BBC
BBCWe are now in the era of weight-loss drugs.
Decisions on how these drugs will be used look likely to shape our future health and even what our society might look like.
And, as researchers are finding, they are already toppling the belief that obesity is simply a moral failing of the weak-willed.
Weight-loss drugs are already at the heart of the national debate. This week, the new Labour government suggested they could be a tool to help obese people in England off benefits and back into work.
That announcement – and the reaction to it – has held a mirror up to our own personal opinions around obesity and what should be done to tackle it.
Here are some questions I’d like you to ponder.
Is obesity something that people bring on themselves and they just need to make better life choices? Or is it a societal failing with millions of victims that needs stronger laws to control the types of food we eat?
Are effective weight-loss drugs the sensible choice in an obesity crisis? Are they being used as a convenient excuse to duck the big issue of why so many people are overweight in the first place?
Personal choice v nanny state; realism v idealism – there are few medical conditions that stir up such heated debate.
I can’t resolve all those questions for you – it all depends on your personal views about obesity and the type of country you want to live in. But as you think them over, there are some further things to consider.
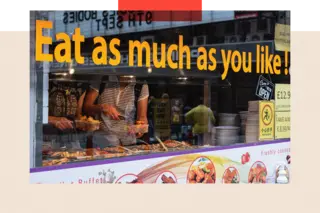
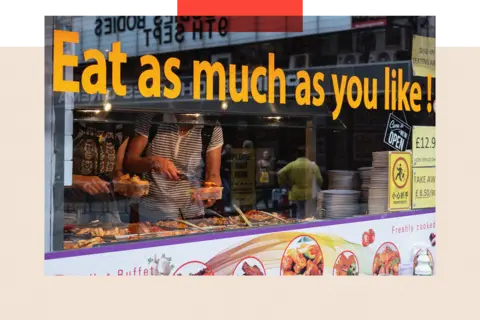
Obesity is very visible, unlike conditions such as high blood pressure, and has long come with a stigma of blame and shame. Gluttony is one of Christianity’s seven deadly sins.
Now, let’s look at Semaglutide, which is sold under the brand name Wegovy for weight loss. It mimics a hormone that is released when we eat and tricks the brain into thinking we are full, dialling down our appetite so that we eat less.
What this means is that by changing only one hormone, “suddenly you change your entire relationship with food”, says Prof Giles Yeo, an obesity scientist at the University of Cambridge.
And that has all sorts of implications for the way we think about obesity.
It also means for a lot of overweight people there is a “hormonal deficiency, or at least it doesn’t go up as high”, argues Prof Yeo, which leaves them biologically more hungry and primed to put on weight than someone who is naturally thin.
That was likely an advantage 100 or more years ago when food was less plentiful – driving people to consume calories when they are available, because tomorrow there may be none.
Our genes have not profoundly changed in a century, but the world we live in has made it easier to pile on the pounds with the rise of cheap and calorie-dense foods, ballooning portion sizes and towns and cities that make it easier to drive than walk or cycle.
These changes took off in the second half of the 20th Century, giving rise to what scientists call the “obesogenic environment” – that is, one that encourages people to eat unhealthily and not do enough exercise.
 Getty Images
Getty ImagesNow one in four adults in the UK is obese.
Wegovy can help people lose around 15% of their starting body weight before the benefits plateau.
Despite constantly being labelled a “skinny drug” this could take someone weighing 20 stone down to 17 stone. Medically, that would improve health in areas like heart attack risk, sleep apnoea and type 2 diabetes.
But Dr Margaret McCartney, a GP in Glasgow, cautions: “If we keep putting people into an obesogenic environment, we’re just going to increase need for these drugs forever.”
At the moment the NHS is planning to prescribe the drugs only for two years because of the cost. Evidence shows that when the injections stop, the appetite comes back and the weight goes back on.
“My big concern is the eye is taken off the ball with stopping people getting overweight in the first place,” says Dr McCartney.
We know the obesogenic environment starts early. One in five children is already overweight or obese by the time they start school.
And we know that it hits poorer communities (in which 36% of adults in England are obese) harder than wealthier ones (where the figure is 20%), in part due to the lack of availability of cheap, healthy food in those less affluent districts.
But there is often a tension between improving public health and civil liberties. You can drive, but you have to wear a seatbelt; you can smoke, but with very high taxes alongside restrictions on age and where you can do it.
So here are some further things for you to consider. Do you think we should also tackle the obesogenic environment or just treat people when it’s starting to damage their health? Should government be far tougher on the food industry, transforming what we can buy and eat?
Should we be encouraged to go Japanese (a rich country with low obesity) and have smaller meals based around rice, vegetables and fish? Or should we cap the calories in ready meals and chocolate bars?
What about sugar or junk-food taxes? What about wider bans on where calorie-dense foods can be sold or advertised?
Prof Yeo says if we want change then “we’re going to have to compromise somewhere, we’re going to have to lose some liberties” but “I don’t think we’ve come to a decision within society, I don’t think we’ve debated it”.
In England, there have been official obesity strategies – 14 of them across three decades and with very little to show for it.
They included five-a-day campaigns to promote eating fruit and veg, food labelling to highlight calorie content, restrictions on advertising unhealthy food to children and voluntary agreements with manufacturers to reformulate foods.
But although there are tentative signs that child obesity in England may be starting to fall, none of these measures have sufficiently altered the national diet to turn the tide on obesity overall.
There is one school of thought that weight-loss drugs may even be the event that triggers the change in our meals.
“Food companies profit, that’s what they want – the only ray of hope I have is if weight-loss drugs help a lot of people resist buying fast foods, can that start the partial reversal of the food environment?” asks Prof Naveed Sattar from the University of Glasgow.
As weight-loss drugs become far more available, deciding how they will be used and how that fits into our wider approach to obesity will need to be addressed soon.
At the moment we are only dipping our toes in the water. There is limited supply of these drugs and because of their huge expense, they are available on the NHS to relatively few people and for a short time.
That is expected to change dramatically over the next decade. New drugs, such as tirzepatide, are on the way and the pharmaceutical companies will lose their legal protections – patents – meaning other companies can make their own, cheaper versions.
In the early days of blood-pressure-lowering medicines or statins to reduce cholesterol, they were expensive and given to the few who would benefit the most. Now around eight million people in the UK are taking each of those drugs.
Prof Stephen O’Rahilly, director of the MRC Metabolic Diseases Unit, says blood pressure was tacked with using a combination of drugs and societal change: “We screened for blood pressure, we advised about lower sodium [salt] in foods and we developed cheap, safe and effective blood pressure drugs.”
That’s analogous, he says, to what needs to happen with obesity.
It is still not clear how many of us will end up on weight-loss medication. Will it only be for those who are very obese and at medical risk? Or will it become preventative to stop people becoming obese?
How long should people take weight-loss drugs for? Should it be for life? How widely should they be used in children? Does it matter if people using the drugs are still eating unhealthy junk food, just less of it?
How quickly should weight-loss medications be adopted when we still do not know the side-effects of long term use? Are we OK with healthy people taking them entirely for cosmetic reasons? Could their availability privately widen the obesity and health gap between rich and poor?
So many questions – but, as yet, few clear answers.
“I don’t know where this is going to land – we’re on a voyage of uncertainty,” says Prof Naveed Sattar.
Top picture: Getty Images
BBC InDepth is the new home on the website and app for the best analysis and expertise from our top journalists. Under a distinctive new brand, we’ll bring you fresh perspectives that challenge assumptions, and deep reporting on the biggest issues to help you make sense of a complex world. And we’ll be showcasing thought-provoking content from across BBC Sounds and iPlayer too. We’re starting small but thinking big, and we want to know what you think – you can send us your feedback by clicking on the button below.







